
The Paperwork Just Changes Accents
$27 million to Republicans. $25 million to Democrats. Same industry. Same cycle. Same math.

By Markus Grant | The Ranter
Health sector PACs gave $27 million to Republicans and $25 million to Democrats in the 2023-2024 election cycle. [1] That is not a typo. The split is 52 to 48. In an industry that depends on federal reimbursement rates set by Congress, the money does not pick a side. It picks both sides. Evenly. On purpose.
The American Hospital Association spent $32 million lobbying Congress in 2025. [2] Over the prior twelve months, 18 rural hospitals closed or converted. I am not saying those two numbers are related. I am saying they exist in the same sentence and nobody in Washington seems to find that interesting.
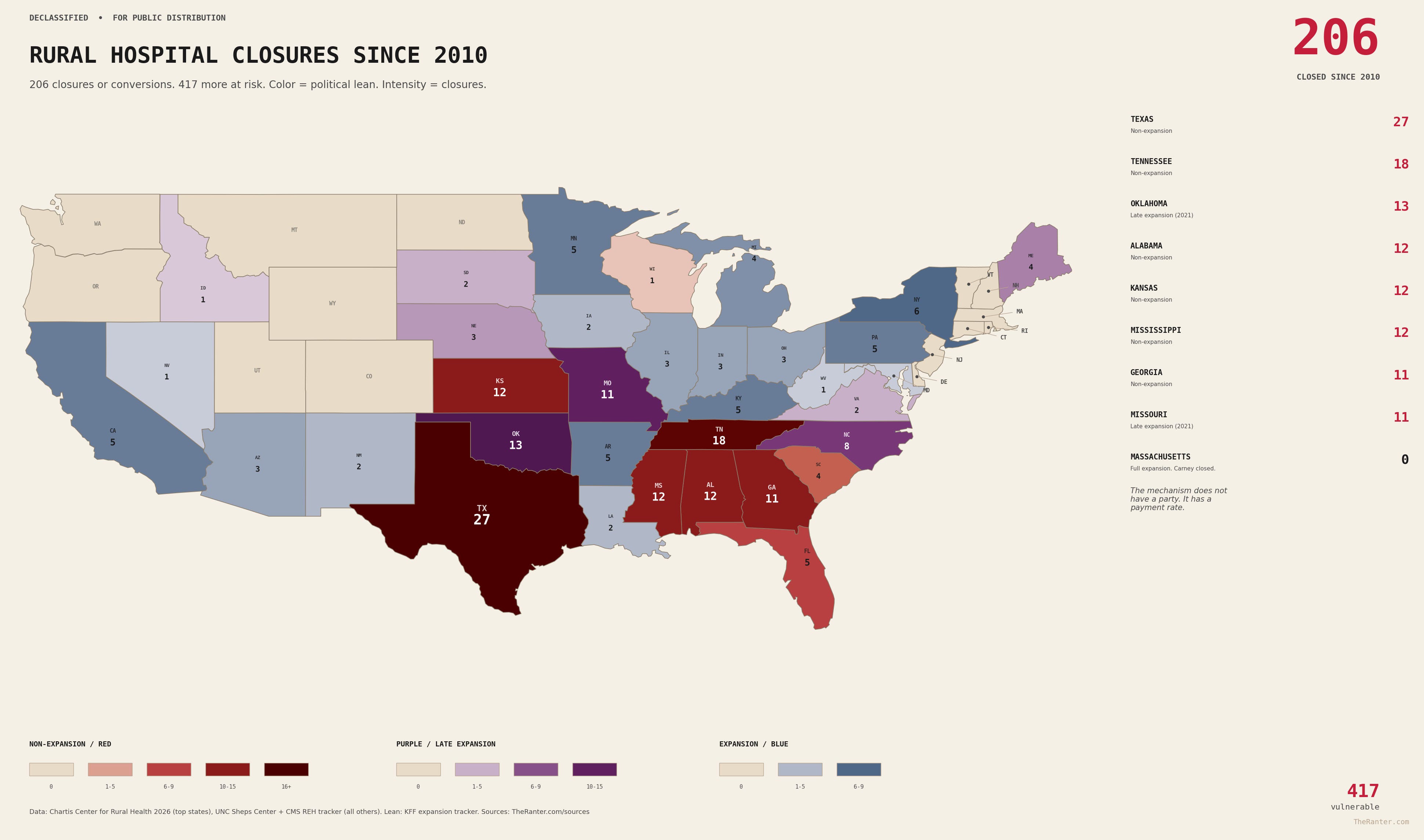
Medicare pays hospitals 83 cents for every dollar it costs to treat a patient. Medicaid pays 88 cents. Rural hospitals see more of those patients than anyone else, and they lose money on nearly all of them. Private equity bought the struggling ones, extracted hundreds of millions, and left the debt behind. More than 200 rural hospitals have closed or converted since 2010. The math was broken. The investors monetized the break. Nobody in Washington fixed either one.
This article is about why.
The easiest version of this story is the one where you blame one party. It is also the wrong one.
Start with the states that refused Medicaid expansion. Seventy-four percent of all rural hospital closures between 2010 and 2021 occurred in states that had not expanded Medicaid or had expanded it for less than a year. [3] Texas leads the nation with 27 closures or conversions. Tennessee, Oklahoma, Mississippi, Alabama, Kansas. The pattern is not subtle.
In Tennessee, there was a plan. Governor Bill Haslam, a Republican, proposed Insure Tennessee in 2014. It was designed for a conservative state. It included work requirements. It had an off-ramp if federal matching funds dropped below a threshold. The state’s hospital associations backed it and agreed to finance the state’s share through an assessment, because they saw it as essential to survival. [4]
Americans for Prosperity spent approximately $300,000 on advertising, town halls, door-to-door canvassing, and phone banking to kill it. Their messaging tied the plan to President Obama and accused Republican lawmakers of breaking their promise to oppose the Affordable Care Act. The plan died in committee. [4]
Tennessee had already lost multiple rural hospitals. By 2018, nine had closed. [4] AFP spent $300,000 to block a plan designed to keep hospitals open. The hospitals closed. The money came from out of state. The closures did not.
In Texas, Governor Greg Abbott rejected Medicaid expansion entirely, calling it a “massive expansion of an already broken and bloated Medicaid program.” [5] Texas built a waiver system instead, one that funds uncompensated emergency care using local hospital district taxes to draw down federal dollars. The structure works for urban hospitals with strong tax bases. Rural districts with weak tax bases got the 83-cent math, plus nothing. Texas has lost more rural hospitals than any state in the country.
The metaphor stayed dry. The counties did not.
Now here is where someone is going to sort this into a partisan bucket and feel finished. Do not get comfortable.
The Affordable Care Act expanded Medicaid coverage. It did not fix the reimbursement rate. Medicare still pays 83 cents. Medicaid still pays 88 cents. No administration, Democratic or Republican, has fixed the underlying gap. The ACA turned zero-dollar patients into 88-cent patients. That is an improvement. It is not a solution. In expansion states, 35 percent of rural hospitals are still operating at a loss. [3]
Massachusetts expanded Medicaid. Massachusetts has a Democratic governor, a Democratic legislature, a Democratic attorney general, and a city council that voted 12 to 0 to try to save Carney Hospital. Carney closed anyway. The coverage was there. The building was not. The reimbursement math does not check voter registration.
The rate is the constant. Expansion is one variable. One side refused the variable and made the math worse. The other side accepted the variable and called it a fix. The math kept running.
One side can refuse Medicaid expansion and make the hole deeper. The other side can preserve the hole and call it a compromise. The hole appreciates the nuance.
This past July, the One Big Beautiful Bill became law. The Congressional Budget Office estimates it cuts Medicaid and ACA spending by more than $1 trillion over ten years and leaves approximately 10 million more people uninsured. [6]
The same law includes a $50 billion Rural Health Transformation Program. Five years of funding. Ten billion a year. On paper, that sounds like an offset. It is not.
The NRHA and Manatt Health project that rural hospitals will lose approximately 21 cents of every Medicaid dollar they currently receive. [7] The fund does not cover the cuts it was designed to offset. They named it after the thing it does not do.
States can only devote 15 percent of RHTP funds to direct patient care payments. The rest must go to “innovative projects and technologies.” Rural hospital associations in Colorado, Michigan, and Nebraska stated publicly that the program will not save a single hospital. [8] Transformation is a lovely word when you are trying not to say subtraction.
The fund was not enough. Then it got conditions.
By December 2025, the administration began distributing RHTP funds with conditions. Twelve billion dollars of the five-year total is tied to whether states implement health policies aligned with the Make America Healthy Again initiative, including banning the use of SNAP benefits for certain foods and requiring schools to participate in the Presidential Fitness Test. The administration can claw back funds annually if states do not deliver on promised policies. [9]
The rural hospital fund is now a policy lever. The hospitals are the collateral.
It is already happening. In northeast Georgia, a hospital closed its maternity ward. In rural New Hampshire, a community health center shuttered. In Iowa, a Des Moines hospital system laid off employees and closed a clinic. Hospitals are not waiting for the Medicaid provisions to take full effect. They are cutting now, because the math is already moving. [10]
Rep. Jodey Arrington of Texas is the House Budget Committee chair. The Texas Observer calls him the “House architect” of the One Big Beautiful Bill. [11]
Arrington’s district covers rural West Texas. It contains 25 rural hospitals. Six of those hospitals are categorized as at risk of closing. [11]
He received $13,000 from AHA-linked sources in the 2024 cycle while designing the bill. [11] Thirteen thousand dollars. That is not a bribe. That is a rounding error in a PAC budget, and it did not need to be more than that, because the system does not run on bribes. It runs on access. The money does not buy the vote. It buys the meeting. The meeting is where the math gets set.
Down in Alabama, ALEC published an op-ed in Yellowhammer News arguing that Medicaid expansion is a “mirage” that will not save the state’s rural hospitals. [12] Alabama has had five or more rural hospital closures since 2010. Alabama still has not expanded Medicaid. Peer-reviewed studies consistently find that expansion improves rural hospital finances and reduces closure probability.
They called the solution a mirage in the state that most needs the water.
I want to be precise about what this article is saying, because it would be easy to read it as “both sides are the same” and move on. That is not the claim.
The states that refused expansion made the crisis measurably worse. That is documented. Seventy-four percent of closures in non-expansion states is not a coincidence. AFP spending $300,000 to kill a plan that Tennessee hospitals said would keep them alive is not a policy disagreement. It is a receipt.
But the reimbursement rate that makes rural hospitals structurally unprofitable has survived every administration since it was set. Democratic congresses have not raised it. Republican congresses have not raised it. The AHA has spent over $90 million lobbying in the last three years and the rate has not moved. [2] The PAC money flows to both parties because the system serves both parties. Not as a conspiracy. As an equilibrium.
Health sector PACs gave $25 million to Democrats and $27 million to Republicans. [1] That is not conviction. That is portfolio management.
The country argues red versus blue while the money behaves like beige.
This is the last of four articles I wrote about why rural hospitals close. The reimbursement math. The private equity extraction. A specific hospital in a specific neighborhood. And now the political money that keeps all of it in place.
The mechanism does not have a party. It has a payment rate, a lobbying budget, and a PAC split that covers its bets. One side can refuse to expand coverage and accelerate the closures. The other side can expand coverage and leave the rate untouched. The hospital closes either way. The paperwork just changes accents.
417 rural hospitals are flagged as financially vulnerable right now. [3] The number has not gotten smaller in a decade. The reimbursement rate has not gotten higher. The lobbying spend has not gotten lower. The PAC split has not gotten less even.
If you are waiting for me to tell you whose fault this is, I cannot do that. Not because I do not have opinions. Because the receipts do not support a clean answer. The receipts support a system. The system does not need a villain. It needs both teams to keep playing, and both teams keep showing up, and the check clears either way.
The math was not designed to close rural hospitals. It was designed for a system where someone else would cover the difference. In a rural county where the median age is 58 and the largest employer left in 2009, there is no one else.
In Washington, where the PAC checks arrive on time and the lobbying meetings stay on the calendar, there is everyone else. They just have somewhere else to be.
Sources
[1] OpenSecrets: Health Sector PAC Contributions, 2023-2024 Cycle. Total: $52.2 million. Democrats: $25.0 million. Republicans: $27.0 million.
[2] OpenSecrets: American Hospital Association Federal Lobbying. 2023: $30.2 million. 2024: $29.0 million. 2025: $32.0 million.
[3] Chartis Center for Rural Health: 2026 State of the State. 417 vulnerable rural hospitals. In non-expansion states: 52.2% operating at a loss. In expansion states: 34.9% operating at a loss. 74% of closures in non-expansion states, 2010-2021 (AHA fact sheet). Texas: 27 closures or conversions.
[4] NBC News: Koch Group Shows Its Power in Tennessee, February 2015. AJMC: Why Did Tennessee’s Medicaid Expansion Plan Fail?. Tennessee hospital closure data from UNC Sheps Center.
[5] Texas Tribune: Abbott Holds Firm Against Medicaid Expansion, April 2015. Texas Tribune/Public Health Watch: Why Do Texas Republicans Still Oppose Medicaid Expansion?, November 2022.
[6] KFF: Health Provisions in the 2025 Federal Budget Reconciliation Law. CBO: One Big Beautiful Bill Act Analysis. CBO projects $1+ trillion in Medicaid/ACA spending reductions and 10 million increase in uninsured by 2034.
[7] NRHA and Manatt Health: H.R. 1 and RHTP Advocacy. Rural hospitals projected to lose 21 cents of every Medicaid dollar. NC Health News: Rural Health Transformation Program Won’t Make Up for Federal Budget Cuts.
[8] KFF Health News: Lawmakers, Health Groups Resist State Rural Health Fund Plans, March 2026. CBS News: State Rural Health Transformation Plans. 15% direct patient care cap per RHTP statute.
[9] PBS NewsHour: Trump Administration Rolls Out Rural Health Funding, With Strings Attached, December 29, 2025. $12 billion of RHTP tied to MAHA policy priorities. Annual recalculation with clawback authority.
[10] CNN: Hospitals Are Making Cuts After ‘Big Beautiful Bill,’ Fueling Midterm Fears, March 2, 2026. Georgia maternity ward closure, New Hampshire health center closure, Iowa layoffs and clinic closure.
[11] Texas Observer: West Texas Congressman’s ‘Big Beautiful’ Cuts Could Harm Rural Hospitals in His District, September 2025. OpenSecrets FEC data. Sheps Center analysis. Rep. Jodey Arrington (R-TX-19): 25 rural hospitals in district, 6 at risk. $13,000 from AHA-linked sources, 2024 cycle.
[12] Yellowhammer News: Alabama’s Hospital Crisis and The Medicaid Expansion Mirage, April 2024. ALEC op-ed by Brooklyn Roberts and Rep. Arnold Mooney. Georgetown CCF and Health Affairs studies on expansion and rural hospital financial performance.
Another eye-opening article.