
The Hospital That Was Designed to Fail
More than 200 hospitals closed. The formula that killed them hasn't changed.

When a rural hospital closes, the ambulance has to drive farther. It sounds obvious, but the number is worth saying out loud.
Before a closure, the average ambulance transport in a rural area takes 14.2 minutes. After the hospital shuts down, that number jumps to 25.1 minutes.[1] Eleven extra minutes. During a stroke, brain cells die at roughly 1.9 million per minute, and every minute of delay shrinks the window for the one drug that can reverse it. During a car accident on a two-lane road at 11 PM, eleven minutes is the difference between an ER and a helicopter.
Since 2010, more than 200 rural hospitals have closed or converted to models that no longer include inpatient care.[2] Not “are struggling.” Not “facing headwinds.” Closed. Doors locked. Signs dark. Ambulances rerouted. Eighteen of those closures or conversions happened in the last year alone. Another 417 are currently flagged as financially vulnerable.[3] That is roughly one in four rural hospitals in the country sitting on a list that has not gotten shorter in a decade.
There is a version of this story that is about politics. This one is about the math that made the politics necessary.
The federal government pays hospitals for treating Medicare patients through something called the Prospective Payment System. In plain English: Medicare decides in advance what your appendix costs. If the actual cost of removing your appendix in a rural county with one surgeon, one anesthesiologist, and a supply chain that runs through a single distributor is higher than what Medicare decided, Medicare does not adjust. The price was set. You eat the difference.
Medicare pays hospitals 83 cents for every dollar it actually costs to treat a patient. Medicaid pays roughly 88 cents. In 2023, combined underpayment across all U.S. hospitals topped $130 billion.[4]
That is not a rounding error. That is the system working the way it was built.
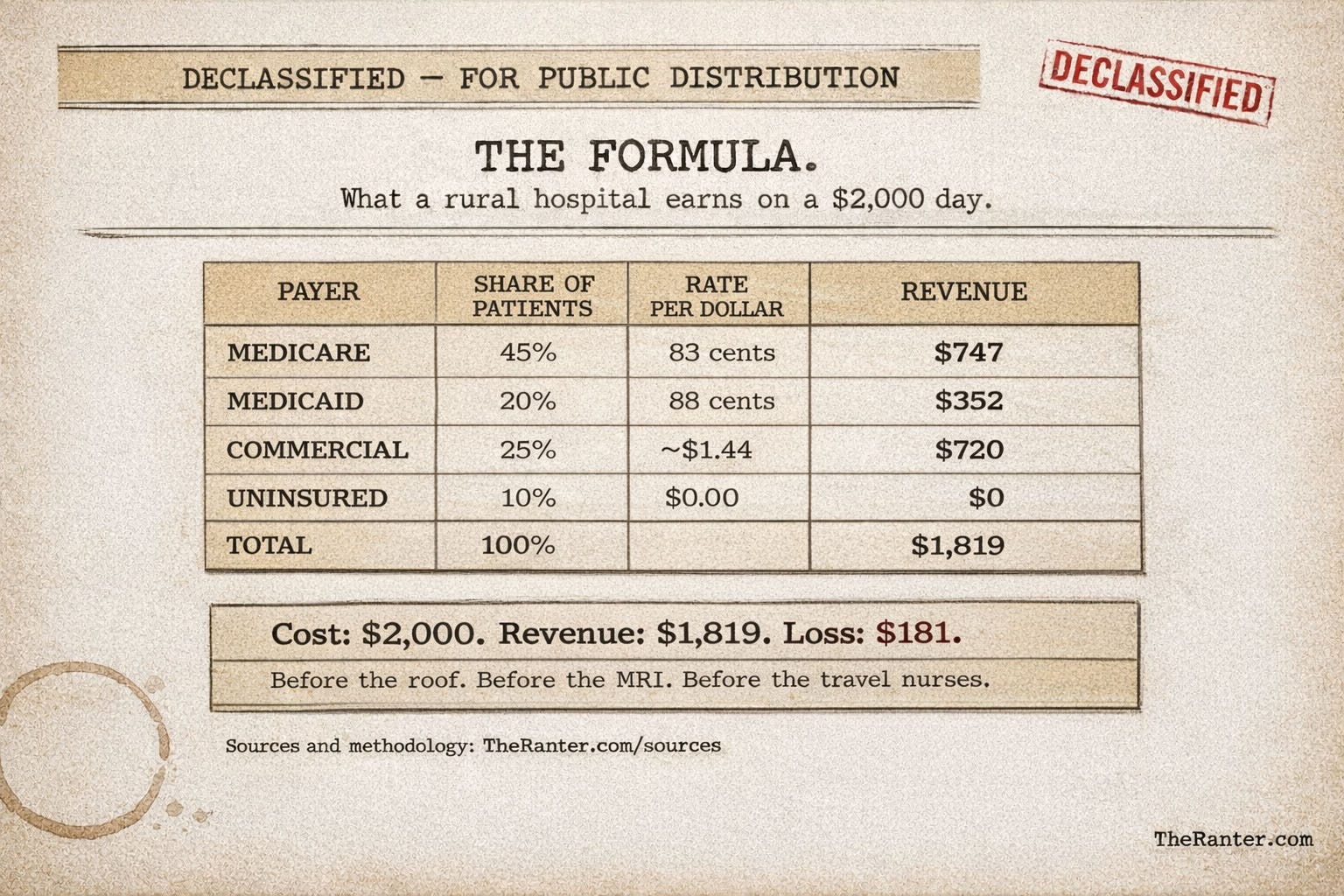
Now put that math inside a rural hospital. A typical rural facility sees a patient mix that looks something like this: 45% Medicare, 20% Medicaid, 25% commercial insurance, 10% uninsured. The commercial patients are the only ones who pay above cost. They subsidize the losses from everyone else. In a city hospital, that commercial share might be 40% or higher. Enough cushion to absorb the Medicare and Medicaid shortfall and still keep the lights on.
Rural hospitals do not have that cushion. The population is older, which means more Medicare. It is lower-income, which means more Medicaid. The commercial base is small because the employers are small. You cannot negotiate higher commercial rates when you have no bargaining power, and you cannot raise volume when your population is shrinking.
Rural hospitals are not failing because nobody needs them. They are failing because the people who need them most are covered by programs that pay below cost, and the people with commercial insurance are too few to cover the gap. The math was always going to produce a loss.
Assume a cost of $2,000 per inpatient day. Apply the payer mix. Apply the reimbursement ratios. The expected revenue per day comes out to roughly $1,820.[5]
That is a loss of about $180 per patient per day. Before capital costs. Before the roof repair. Before the MRI machine that needs replacing. Before the travel nurses you are paying a premium for because nobody wants to relocate to a county with one traffic light and a Dairy Queen.
More than 40% of rural hospitals are currently operating in the red.[3] The question is not why so many are closing. The question is how any of them are still open.
There is a federal designation called Critical Access Hospital. It exists because someone in Washington looked at this math and realized it was going to kill rural hospitals. The fix: if your hospital has fewer than 25 inpatient beds, is more than 35 miles from the nearest other hospital, and keeps the average patient stay under 96 hours, you qualify, and Medicare pays you 101% of your actual costs instead of the standard rate.[6]
There are about 1,350 hospitals with this designation. For them, the Medicare piece of the math is solved. Not generously. One percent above cost is not a windfall. But it stops the bleeding on the Medicare side. The other rural hospitals get 83 cents. Critical Access status pays 101 percent of cost for Medicare patients, which sounds generous until you notice how many hospitals are too close to qualify and too small to survive the regular formula.
Two problems.
First, not every rural hospital qualifies. If you are 20 miles from the next facility instead of 35, you are too close. You serve a town of 800 people with a median age of 58, and your ER handles everything from chest pain to farming accidents. But because there is another hospital 20 miles down the highway, you get the standard rate. 83 cents on the dollar. Congress noticed. A bipartisan bill in early 2026 proposed letting HHS grant cost-based reimbursement to hospitals that function as the sole provider for their community, regardless of the 35-mile rule.[14] The map says you are close to another hospital. The road says otherwise.
Second, the 96-hour rule. Rural hospitals now manage more complex patients than they used to. The population is older. Chronic conditions are more common. Post-surgical recovery takes longer. But if the average patient stay goes over 96 hours, the hospital risks losing its CAH designation. So they transfer patients out. The policy designed to keep rural hospitals alive creates a rule that pushes patients away from them.
Here is where someone is going to sort this into a political bucket. Let them try.
Seventy-four percent of all rural hospital closures between 2010 and 2021 occurred in states that had not expanded Medicaid.[7] Texas leads the nation with 27 closures or conversions. Tennessee has lost 18. Oklahoma, Mississippi, Kansas: a dozen or more each.[2] These are states where the federal government offered to cover low-income adults at 90 cents on the federal dollar, and the state said no. The uninsured patients kept showing up. The hospital treated them and got paid nothing. In the states that still have not expanded, more than half of rural hospitals are operating in the red.[3] Zero is worse than 88 cents.
That is a real and documented pattern. I am not going to pretend it is not there.
But the math underneath does not check voter registration.
Maine has the oldest population in the country: 23.5% of its residents are 65 or older.[9] Vermont is second at 22.9%. New Hampshire is at 21.5%. These are not retirement states in the way Florida is a retirement state. These are states where people aged in place because nobody came to replace them. Younger workers left. The population got older. The payer mix followed.
When nearly a quarter of your patients are on Medicare, and Medicare pays 83 cents on the dollar, expansion does not fix that. You can expand Medicaid all day. Maine did, in 2019. Vermont and New Hampshire did in 2014. The uninsured rate dropped, and the hospitals kept losing money, because the problem was never only about who has insurance. The problem is what insurance pays.
In 2015, two Maine hospitals closed their inpatient units: Parkview Adventist in Brunswick and Southern Maine Health Care in Sanford.[10] Both in an expansion state. Both with Medicaid on the books. Both unable to make the math work with a patient base that was old, publicly insured, and shrinking. In central Massachusetts, Baystate Mary Lane Hospital in Ware closed its inpatient services in 2016 and completed a years-long conversion to outpatient-only care.[11] The inpatient census was too low to justify the overhead. The community did not lose a hospital to a political decision. They lost it to a spreadsheet.
Connecticut has three rural hospitals. All three are operating in the red.[12] Zero closures. Not because the system is working. Because there are only three left to lose.
New Hampshire has not lost a rural hospital in two decades. But four are currently at risk, three at immediate risk.[13] The state expanded Medicaid. The hospitals stayed open, and the math still does not work, because the payer mix is old and the reimbursement rate does not care what state you are in.
Expansion helps. It turns zero-dollar patients into 88-cent patients. But the reimbursement math was set before the expansion debate started. The states that refused expansion made the math worse. The states that accepted it did not make the math good. In expansion states, 35% of rural hospitals are still operating at a loss.[3]
The 74% stat is real, and it matters. But if you look at it and think “this is a red state problem,” you have missed the mechanism. The mechanism is the payment rate. Expansion is one variable. The rate is the constant.
Rural hospital closures increase inpatient mortality by a relative 8.7% in the communities they leave behind.[8] No comparable mortality effect in urban areas. The ambulance time is part of it. The loss of inpatient beds, surgery, maternity care, and behavioral health services is the rest. More than 300 rural hospitals have eliminated obstetric services in the last decade.[3] When the nearest delivery room is an hour away, some women make it. The data says not all of them do.
This is the first of four articles. I started here because the math has to come first. If you do not understand the reimbursement structure, the rest of the story does not make sense. You will see greed, politics, and incompetence in what comes next, but they all sit on top of the same equation. Every hospital that closed, every investor who showed up with a rescue plan, every lobbyist who wrote a check: they all started with this math.
The math was not designed to close rural hospitals. It was designed for a system where someone else would cover the difference. In a rural county where the median age is 58 and the largest employer left in 2009, there is no one else. The math just runs.
The next article is about what happened when private investors showed up and offered to help.
Sources
[1] Troske, S., Davis, A.F. “Do Hospital Closures Affect Patient Time in an Ambulance?” Rural and Underserved Health Research Center, University of Kentucky, 2019.
[2] Chartis Center for Rural Health, “2026 State of the State,” February 2026. 206 rural hospitals closed or converted since 2010. State-level closure counts: Texas (27), Tennessee (18), Oklahoma (13), Kansas (12), Mississippi (12).
[3] Chartis Center for Rural Health, “2026 State of the State” and “2025 State of the State.” 417 vulnerable rural hospitals, 41.2% operating at a loss. Non-expansion states: 52.2%. Expansion states: 34.9%. More than 300 rural hospitals eliminated OB services between 2011 and 2024.
[4] American Hospital Association, “The Cost of Caring,” April 2025 and March 2026. Medicare 83 cents per dollar (2023 and 2024 data). Combined Medicare/Medicaid underpayment: $130 billion in 2023.
[5] Constructed from AHA payment-to-cost ratios and MACPAC rural hospital payer mix data. Updated with 2024 Medicare ratio (83 cents).
[6] CMS Critical Access Hospital designation and eligibility requirements. HRSA CAH program. MedPAC March 2024 Report to Congress.
[7] American Hospital Association, “Medicaid Coverage Supports Rural Patients, Hospitals, and Communities.” Fact sheet, March 2026. 74% of closures in non-expansion states, 2010-2021.
[8] Gujral, K. and Basu, A. “Impact of Rural and Urban Hospital Closures on Inpatient Mortality.” NBER Working Paper 26182, 2019.
[9] U.S. Census Bureau, 2024 Population Estimates. Maine: 23.5% age 65+ (highest nationally). Vermont: 22.9%. New Hampshire: 21.5%.
[10] UNC Cecil G. Sheps Center for Health Services Research. Rural Hospital Closures database. Parkview Adventist Medical Center and Southern Maine Health Care, inpatient services ceased 2015.
[11] Baystate Health / Mary Lane Hospital, Ware, MA. Inpatient services ceased 2016. Outpatient conversion completed; facility closed 2023.
[12] Chartis Center for Rural Health, “2025 State of the State.” Connecticut: 3 rural hospitals, all operating with negative margins. Confirmed in 2026 report.
[13] Center for Healthcare Quality and Payment Reform (CHQPR). Rural hospitals at risk analysis, verified through December 2025. New Hampshire: 4 rural hospitals at risk, 3 at immediate risk.
[14] Sustaining Rural Healthcare Act. H.R.7727, 119th Congress. Introduced February 2026.