
That $1,900 "Skin-to-Skin" Bill Probably Isn't Real
But a real one exists: $39.35 on a 2016 C-section bill. That single line gives away why your whole birth bill is fiction.

THE RANTER FILES | Markus Grant
There’s a video going around. A social worker reads a hospital bill out loud and stops on a line: skin-to-skin contact, $1,900. A charge, they say, for a new mom to hold her own baby. It is the kind of clip built to make your blood boil before it finishes so I fact check it before I become outraged.
I went down the rabbit hole and here is what I found. The Daily Dot, which ran the clip, says straight out that it could not verify the bill, the hospital, or the charge. It’s a reenacted phone call. No itemized bill on screen. So the honest move is to set the $1,900 aside and go find one that’s real.
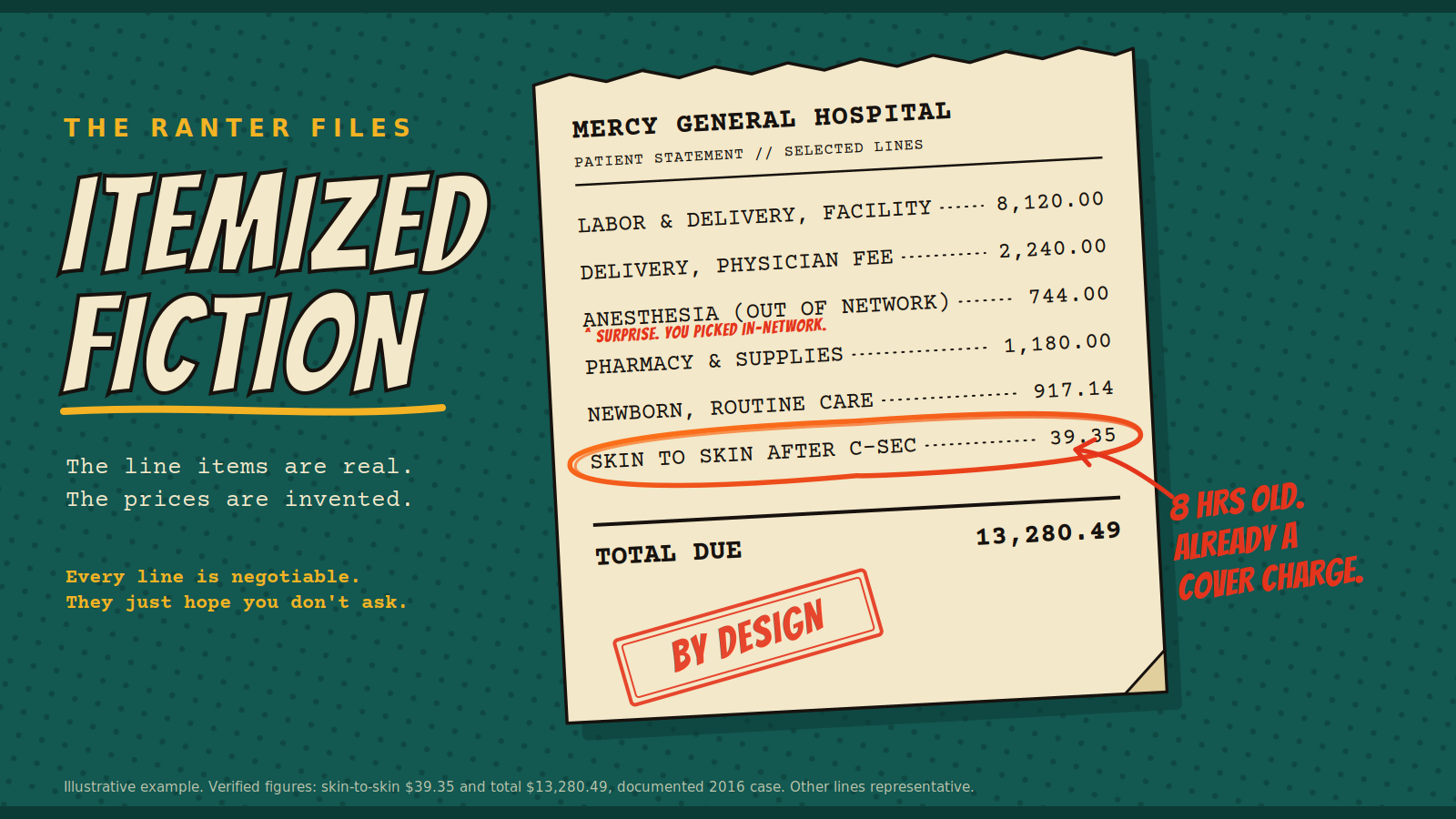
In 2016 a dad in Spanish Fork, Utah, posted his wife’s itemized bill after a C-section at Utah Valley Hospital. $13,280.49, and buried in it, a line reading “skin to skin after C-sec,” $39.35. He wasn’t even angry. He thought it was funny and started a joke fundraiser to cover the forty bucks. The kid had been alive about eight hours and already owed a cover charge to be held by his own mother. We spent a couple generations making everybody soft, and the pendulum apparently swung so far the other way it started billing newborns for a hug.
A doula named Meaghan Grant (no relation) wrote a post that went around explaining it. During a C-section the mother is flat on a narrow table, arms out for IV lines, medicated. If you want the baby on her chest safely, someone has to be there to hold that baby and watch her. That someone is an extra nurse. The charge, the hospital said, was for the nurse, not for the holding. Fair enough. Nurses are the biggest line in any hospital budget, and their time is worth paying for.
So why does the whole thing still seem like a hustle? Because a good reason for the nurse does not make the bill honest.The dishonest half is the part nobody films.
I have read enough of these bills to tell you a birth is never one bill. It’s three, showing up on their own schedules from their own networks. The hospital charges a facility fee off its chargemaster, a master price list the hospital sets and negotiates differently with every insurer, with almost no fixed link to what anything costs. Your obstetrician sends a separate professional fee. Then the anesthesiologist, the one person you did not pick and could not have picked while you were in labor, turns up on a third bill, often from outside your network entirely.
A study in JAMA Health Forum tracked more than 95,000 privately insured families who delivered at in-network hospitals in 2019. Nearly one in five still got a surprise out-of-network bill, about $744 at the middle. The single most common trigger was anesthesia. You booked in-network, and the hospital sent in an out-of-network provider at the exact moment you were in no shape to ask questions.
Itemized billing was sold to you as transparency, a way to see what you paid for. Instead it became a menu the hospital orders from, one line at a time, and “skin to skin” is just the line that photographs well. The in-network and out-of-network split was sold as cost control. It became the trapdoor. And the surprise bill isn’t some error the hospital is embarrassed about, because hospitals run entire revenue-cycle departments built around exactly these charges, which is not something you staff up for a mistake.
The No Surprises Act that banned most of these childbirth surprise bills passed Congress with both parties voting yes, and took effect in January 2022 under a rule the Biden administration wrote. It helped. It also left gaps, providers it didn’t cover, consent forms that waive the protection, and hospital consolidation kept climbing under presidents of both parties, because the hospital systems and the insurers write checks to both of them. Follow the money and it doesn’t pick a side.
I am not going to leave you sitting in the anger, so here is what works. When the bill comes, don’t pay off the summary. Call and demand the itemized bill, every line, every code, and read it. Anything tied to anesthesia, neonatology, radiology, or pathology at an in-network hospital is very likely protected under the No Surprises Act, so if you’re being balance-billed for it, say those words and push back. Ask the hospital for the cash or self-pay price on the facility charges, which usually comes in well under the sticker. The bill is a first offer. Treat it like one.
If you want the full teardown of how the chargemaster works, I took it apart in Your Hospital Bill is Wrong.
And if you want the receipt in your inbox every couple of days, that’s what the subscribe button is for.